Check out the FAQ,Terms of Service & Disclaimers by clicking the
link. Please register
to be able to post. By viewing this site you are agreeing to our Terms of Service and Acknowledge our Disclaimers.
FluTrackers.com Inc. does not provide medical advice. Information on this web site is collected from various internet resources, and the FluTrackers board of directors makes no warranty to the safety, efficacy, correctness or completeness of the information posted on this site by any author or poster.
The information collated here is for instructional and/or discussion purposes only and is NOT intended to diagnose or treat any disease, illness, or other medical condition. Every individual reader or poster should seek advice from their personal physician/healthcare practitioner before considering or using any interventions that are discussed on this website.
By continuing to access this website you agree to consult your personal physican before using any interventions posted on this website, and you agree to hold harmless FluTrackers.com Inc., the board of directors, the members, and all authors and posters for any effects from use of any medication, supplement, vitamin or other substance, device, intervention, etc. mentioned in posts on this website, or other internet venues referenced in posts on this website.
We are not asking for any donations. Do not donate to any entity who says they are raising funds for us.
Announcement
Collapse
No announcement yet.
Anti-NMDA receptor encephalitis and other emerging autoimmune brain diseases
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
Autoimmunity and the basal ganglia: new insights into old diseases
Sydenham's chorea (SC) occurs weeks or months after Group A streptococcal infection, and is characterized by involuntary, purposeless movements of the limbs, in addition to behavioural alteration. There is a body of evidence which suggests that SC is an immune‐mediated brain disorder with regional localization to the basal ganglia. Recent reports have suggested that the spectrum of post‐streptococcal CNS disease is broader than chorea alone, and includes other hyperkinetic movement disorders (tics, dystonia and myoclonus). In addition, there are high rates of behavioural sequelae, particularly emotional disorders such as obsessive‐compulsive disorder, anxiety and depression. These findings have lead to the hypothesis that similar immune‐mediated basal ganglia processes may be operating in common neuropsychiatric disease such as tic disorders, Tourette syndrome and obsessive‐compulsive disorder. This review analyses the historical aspects of post‐streptococcal CNS disease, and the recent immunological studies which have addressed the hypothesis that common neuropsychiatric disorders may be secondary to basal ganglia autoimmunity.
Re: Anti-NMDA receptor encephalitis and other emerging autoimmune brain diseases
Dev Med Child Neurol. 2010 May;52(5):e78-82. Epub 2009 Dec 23. Severe childhood encephalopathy with dyskinesia and prolonged cognitive disturbances: evidence for anti-N-methyl-D-aspartate receptor encephalitis.
Department of Paediatrics, Child Neurology, University Hospital Lausanne, Lausanne, Switzerland.
Abstract
AIM:
We report four cases of acquired severe encephalopathy with massive hyperkinesia, marked neurological and cognitive regression, sleep disturbance, prolonged mutism, and a remarkably delayed recovery (time to full recovery between 5 and 18mo) with an overall good outcome, and its association with anti-N-methyl-d-aspartate (anti-NMDA) receptor antibodies. METHOD:
We reviewed the four cases retrospectively and we also reviewed the literature. RESULTS:
Anti-NMDA receptor antibodies (without ovarian teratoma detected so far) were found in the two children tested in this study. INTERPRETATION:
The clinical features are similar to those first reported in 1992 by Sebire et al.,(1) and rarely recognized since. Sleep disturbance was not emphasized as part of the disorder, but appears to be an important feature, whereas coma is less certain and difficult to evaluate in this setting. The combination of symptoms, evolution (mainly seizures at onset), severity, paucity of abnormal laboratory findings, very slow recovery, and difficult management justify its recognition as a specific entity. The neuropathological substrate may be anatomically close to that involved in encephalitis lethargica, in which the same target functions (sleep and movement) are affected but in reverse, with hypersomnolence and bradykinesia. This syndrome closely resembles anti-NMDA receptor encephalitis, which has been reported in adults and is often paraneoplastic.
</td><td valign="top">
</td></tr><tr><td>THE BASAL GANGLIA</td> <td><table align="right" border="0" cellpadding="0" cellspacing="0"> <tbody><tr> <td></td> <td></td> <td></td> <td></td> <td></td> <td></td> <td></td> </tr> </tbody></table></td> </tr> </tbody></table>
The term "basal ganglia" refers to a group of several structures in the brain: the caudate nucleus, the putamen, the globus pallidus, and the subthalamic nucleus. The substantia nigra, a midbrain structure that has many interconnections with the basal ganglia, is not actually part of this grouping but is often associated with it.
The basal ganglia are involved in a complex loop that connects them to various areas of the cortex. The information from the frontal, prefrontal, and parietal areas of the cortex passes through the basal ganglia, then returns to the supplementary motor area via the thalamus. The basal ganglia are thus thought to facilitate movement by channelling information from various regions of the cortex to the SMA. The basal ganglia may also act as a filter, blocking the execution of movements that are unsuited to the situation
Not all of the circuits involving the basal ganglia are motor circuits, however. Many are instead involved in memorizing and in cognitive and emotional processing. A great deal about the basal ganglia remains unknown. They seem to play a far larger role than just their contribution to motor control.
It's a good site : you have different level : here is the " intermediate level"
Re: Anti-NMDA receptor encephalitis and other emerging autoimmune brain diseases
I agree that is very interesting that Sydenham's chorea could be autoimmune in origin, Anne. Maybe research will lead to treatment that might provide quicker recovery, and/or less relapses.
Here's an article that indicates there could be some differences between the causes for SC and Tourette syndrome and PANDA:
Neurology. 2011 Apr 26;76(17):1508-13. Epub 2011 Mar 16.
Antibody binding to neuronal surface in Sydenham chorea, but not in PANDAS or Tourette syndrome.
Brilot F, Merheb V, Ding A, Murphy T, Dale RC.
Source
Neuroimmunology Group, Institute for Neurosciences and Muscle Research, The Kids Research Institute at the Children's Hospital at Westmead, University of Sydney, Australia. ...
Hopefully they will be able to test for specific antibodies for all these neurological autoimmune disorders and find the best treatments.
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
Autoimmune Limbic Encephalitis as an Emerging Pediatric Condition: Case Report and Review of the Literature
Bl?thnaid McCoy, MB, BCh, MRCPI
The Hospital for Sick Children, Toronto, Ontario, Canada,
Tomoyuki Akiyama, MD
The Hospital for Sick Children, Toronto, Ontario, Canada
Elysa Widjaja, MD
The Hospital for Sick Children, Toronto, Ontario, Canada
Cristina Go, MD
The Hospital for Sick Children, Toronto, Ontario, Canada
Abstract
Limbic encephalitis, first described in the 1960s as a paraneoplastic condition, has emerged as an autoimmune condition, occurring often without evidence of an underlying tumor. Many novel autoantibodies have been identified, and this diagnosis is increasingly being made in the pediatric population. This article reports the case of a 16-year-old boy who presented following gastrointestinal illness with subacute evolution of neuropsychiatric symptoms. Brain magnetic resonance imaging revealed progressive hippocampal signal abnormality and swelling. N-methyl-D-aspartate (NMDA) receptor antibody was detected in serum. The patient responded well to pharmacological immunotherapy but has residual cognitive deficits. The available literature on this condition is reviewed. Limbic encephalitis should be considered in the differential diagnosis in children presenting with encephalopathy, particularly with neuropsychiatric manifestations. Long-term surveillance and close follow-up are required to accurately clarify tumor risk and natural history of this condition in children and balance these factors with risks of radiation exposure through imaging.
Copyright ? 2011 by SAGE Publications
Ideggyogy Sz. 2011 Mar 30;64(3-4):119-25. [Anti-NMDA-receptor encephalitis: description of the syndrome in connection with the first Hungarian patient].
[Article in Hungarian]
Holl?dy K, Cs?bi G, L?ng A, R?zsai B, Kom?romy H, Bors L, Ill?s Z.
Source
In the majority of cases, anti-NMDA (N-methyl-D-aspartate) receptor encephalitis is a severe, but treatable disorder, therefore early diagnosis and adequate therapy are very important. It should be suspected in children and young women, who develop acute psychiatric symptoms and seizures. During the course of the disease severe encephalopathy, agitation, hallucinations, orofacial dyskinesias, prolonged cognitive disturbance, autonomic symptoms can be observed and akinetic mutism develops. EEG shows diffuse slowing. Brain MRI is normal or unspecific. Elevated protein, pleiocytosis and oligoclonal bands can be present in the CSF Detection of NMDA-receptor antibodies in sera or CSF confirms diagnosis. We present the case of a 15-year-old girl, who fully recovered within two months after steroid treatment and repeated plasma exchange. Ovarian teratoma has not been detected.
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
Re: Anti-NMDA receptor encephalitis and other emerging autoimmune brain diseases
Canada's CTV did a report on anti-NMDAR encephalitis. There are two mothers interviewed and at the end of the article, there is a link to one of the mother's support group on Facebook, Anti NMDA receptor Encephalitis in Canada/Encephalite Anti NMDA au Canada. (You'll need to join Facebook to see that group and others. I know there is at least one other active group there.)
Parents warn of mystery illness misdiagnosed in kids
Updated: Sun Sep. 25 2011 20:04:29
CTVNews.ca Staff
The parents of children diagnosed with a rare disease are warning parents and doctors to watch for its confusing symptoms, anxious to spread the word about the new and confusing illness....
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
Breakthrough treatment at Dubai's Welcare Hospital rids 13-year-old of violent outbursts and memory lapses
By Sharmila Dhal, Senior Reporter
Published: 00:00 June 9, 201
Dubai: A 13-year-old Indian girl is on the road to recovery after being successfully treated for a rare disease at a city hospital.
[snip]
"This is a rare and new condition called NMDA Receptor Antibody Encephalitis which was globally discovered around four years ago," claimed Dr Mudit Kumar, Specialist Paediatrician and Neonatologist at Welcare Hospital, who made the diagnosis in what is believed to be a first for the UAE and the region.....
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
Re: Anti-NMDA receptor encephalitis and other emerging autoimmune brain diseases
The articles below are both full text.
Eur J Neurosci. Author manuscript; available in PMC 2011 July 14.
Published in final edited form as:
Eur J Neurosci. 2010 July; 32(2): 298?309.
Published online 2010 July 14. doi: 10.1111/j.1460-9568.2010.07349.x http://www.ncbi.nlm.nih.gov/pmc/arti...7/?tool=pubmed Mechanisms underlying autoimmune synaptic encephalitis leading to disorders of memory, behavior and cognition: insights from molecular, cellular and synaptic studies
Moscato EH, Jain A, Peng X, Hughes EG, Dalmau J, Balice-Gordon RJ.
Source
Department of Neuroscience, University of Pennsylvania School of Medicine, Philadelphia, PA 19104-6074, USA.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3086677/
J Neuropsychiatry Clin Neurosci. Author manuscript; available in PMC 2011 October 1.
Published in final edited form as:
J Neuropsychiatry Clin Neurosci. 2011 Fall; 23(1): 90?97.
doi: 10.1176/appi.neuropsych.23.1.90 The Emerging Link Between Autoimmune Disorders and Neuropsychiatric Disease
Dr. Matthew S. Kayser, Department of Psychiatry, at the University of Pennsylvania in Philadelphia.
Dr. Josep Dalmau, Department of Neurology, at the University of Pennsylvania in Philadelphia.
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
Autoimmune Encephalitis ? New Awareness, Challenging Questions
Published on May 17, 2011
Author: Sarosh R Irani
Specialty: Neurology, Immunology, Neuroscience
Institution: Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, University of Oxford
Address: Oxford, OX3 9TH, United Kingdom
Author: Angela Vincent
Specialty: Neurology, Immunology, Neuroscience
Institution: Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, University of Oxford
Address: Oxford, OX3 9TH, United Kingdom
Abstract: The field of autoimmune encephalopathies has expanded rapidly in the last few years. It is now well-established that a substantial proportion of encephalitides are associated with autoantibodies directed against the extracellular domains of cell-surface proteins which are critical in the regulation of neuronal excitability. These include LGI1, CASPR2, contactin-2 (VGKC-complex antibodies), and the NMDA, AMPA, and GABAB receptors. The clinical importance of these conditions lies in their frequent immunotherapy-response and, less commonly, their association with distinctive tumors. Studies which have examined cohorts of patients defined by these serum antibodies have identified a number of clinical features that have helped understand the core phenotypes of these conditions. In addition, sensitive antibody assays have allowed the expansion of the phenotypes to include a minority of patients with isolated epilepsies or psychoses. There is also evidence that autoimmune encephalitis may progress to adult-onset hippocampal sclerosis. Clinical, and accumulating scientific, data strongly suggest direct pathogenicity of these autoantibodies. The generation of the autoantibody, in some patients, can be explained by the presence of tumors which express their antigenic target. Serum antibody levels are higher than their levels in CSF in the vast majority of cases. However, the majority of patients do not harbor a tumor and the etiology of the disease in these patients is less clear. Below, we suggest models for the etiology and pathogenic mechanisms of these autoantibodies by incorporating concepts such as serum generation of the autoantibodies, the blood-brain barrier, intrathecal antibody production, and prodromal infections.
Full text for this comprehensive article is available at the link.
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
Maramattom BV, Jacob A. N-methyl D-aspartate receptor encephalitis: A new addition to the spectrum of autoimmune encephalitis. Ann Indian Acad Neurol [serial online] 2011 [cited 2011 Dec 1];14:153-7. Available from: http://www.annalsofian.org/text.asp?2011/14/3/153/85872
Abstract
A large proportion of "encephalitis" is caused by unknown agents. Of late, a new category of disorders, "autoimmune encephalitis," has been described, which present with features similar to viral encephalitides. A well-delineated and common entity among this group is the recently described anti-NMDAR encephalitis (NMDARE). Although this entity was initially described in young women harboring ovarian teratomas, it is now characterised as well in children and men. Approximately 60% of the patients have an underlying tumor, usually an ovarian teratoma. In 40% of the patients, no cause can be found (idiopathic NMDARE). NMDARE typically presents with psychiatric features followed by altered level of consciousness, severe dysautonomia, hyperkinetic movement disorders, seizures and central hypoventilation. Orofacial dyskinesias resulting in lip and tongue mutilation are quite common. Seizures, are common and may be difficult to treat. The disease can be confirmed by serum and cerebrospinal fluid anti-NMDAR antibodies. Titers of these antibodies can also guide response to treatment. Tumor removal is necessary if identified, followed by immunological treatment. Intravenous methylprednisolone and immunoglobulins aim to suppress/modulate immune response while plasma exchange attempts to remove antibodies and other inflammatory cytokines. Rituximab and cyclophosphamide aim to suppress antibody production. Recovery is slow and often with neurological deficits if treatment is delayed. With many distinctive clinical features, a specific antibody that aids diagnosis, and early effective treatment with commonly available drugs leading to good outcomes, NMDARE is a diagnosis that should be considered early in any case of "unexplained encephalitis."
The article above is another new comprehensive overview of N-methyl D-aspartate receptor encephalitis, (NMDARE). The full text is available.
The last sentence is very interesting:
The similarity of this illness to "encephalitis lethargica" or Japanese B encephalitis [JE] is striking, and presumed JE cases with negative serology should be further investigated to rule out NMDARE.
The article also notes that the first cases of NMDARE were described in Japan. It made me wonder if most cases are appearing in the summer when mosquitoes are out. I'm sure that would have been noticed by now, though.
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
It looks interesting and supports the similarities between the current NMDARE cases and the early 20th century EL epidemic. They mention just cases in young children of both sexes in the EL epidemic, so that leaves out the NMDARE cases predominantly in teen girls and young women today, (many of those having teratomas.)
Perhaps there were less teratomas back in the early 1900's, or there was a bias for diagnosing young women with the symptoms as having strictly non-medical psychiatric problems rather than underlying neurological problems.
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
Prim Care Companion CNS Disord. 2011; 13(4): PCC.10l01141.
doi: 10.4088/PCC.11l01141
PMCID: PMC3219522
Copyright ? 2011, Physicians Postgraduate Press, Inc. The Horse With Stripes: A Case of Anti?NMDA Receptor Encephalitis
Lynn Yen, MD, Margaret Leung, MD, MPH, Denise C. Kellaher, DO, Oladipo Kukoyi, MD, MS, and Glen Xiong, MD
Residency Programs in Family Medicine/Psychiatry (Dr Yen) and Internal Medicine/Psychiatry (Dr Leung) and Departments of Psychiatry and Behavioral Sciences (Drs Kellaher, Kukoyi, and Xiong) and Internal Medicine (Dr Xiong), University of California, Davis, Sacramento
To the Editor: Anti?N-methyl-D-aspartate (NMDA) receptor encephalitis, although rare, is an emerging cause of catatonia.1 We describe a 22-year-old male patient whose akinetic catatonia responded to intravenous immunoglobulin therapy and steroid therapy after his cerebrospinal fluid and serum samples tested positive for the anti-NMDA antibody.
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.) Never forget Excalibur.
 Tweet
Tweet


 </td> <td>
</td> <td> </td> <td>
</td> <td> </td> <td>
</td> <td> </td> </tr> </tbody></table></td> </tr> </tbody></table>
</td> </tr> </tbody></table></td> </tr> </tbody></table> 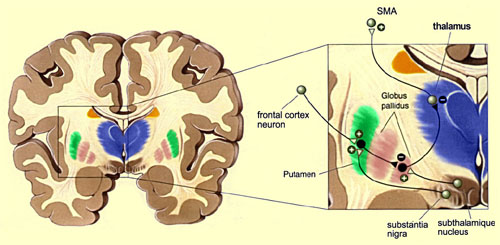
Comment